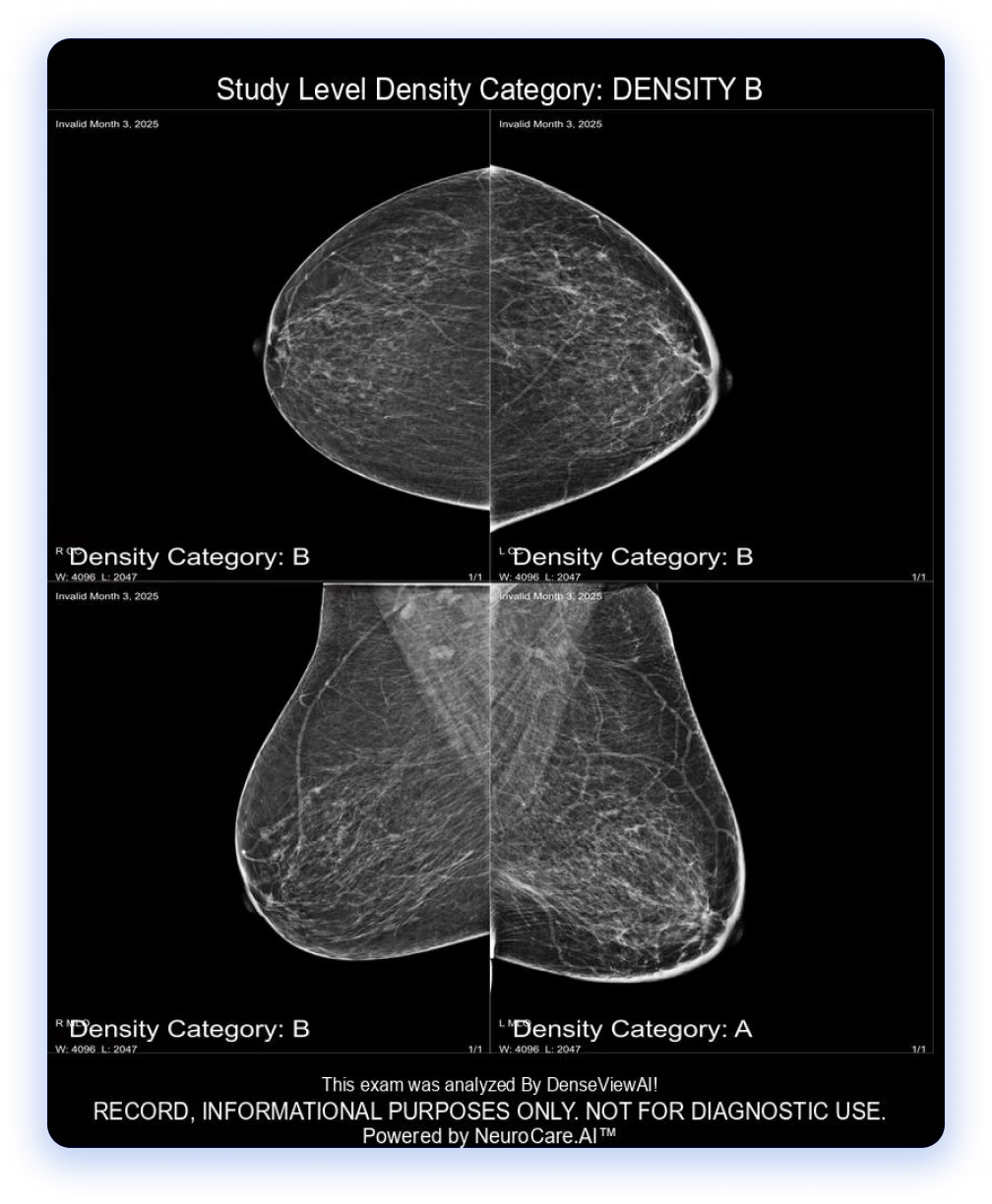
Analyzing screening and diagnostic mammograms for comprehensive breast density assessments.
Approval in Progress!
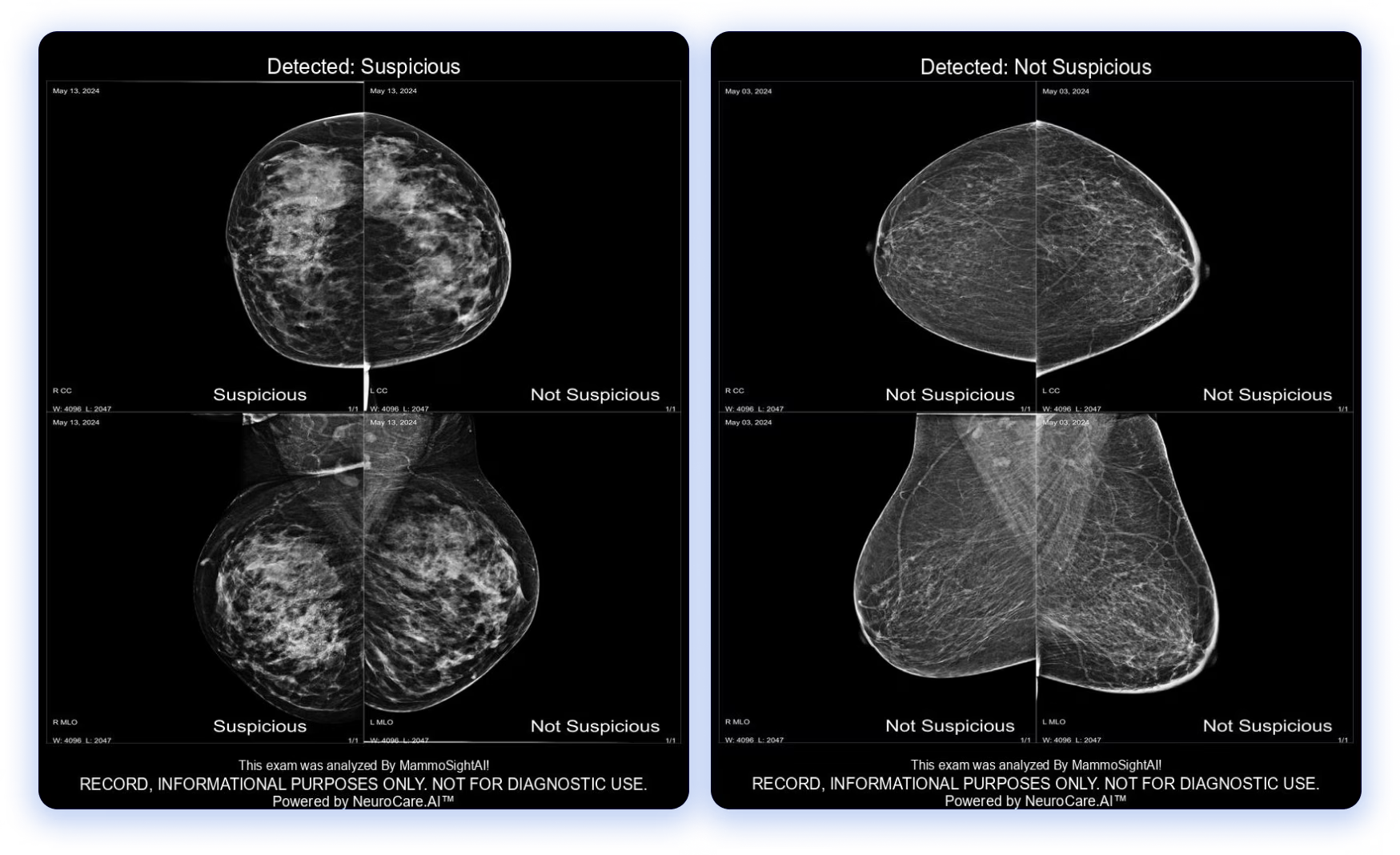
Identifying more cancers faster, improving patient outcomes and streamlining workflows across imaging centers.
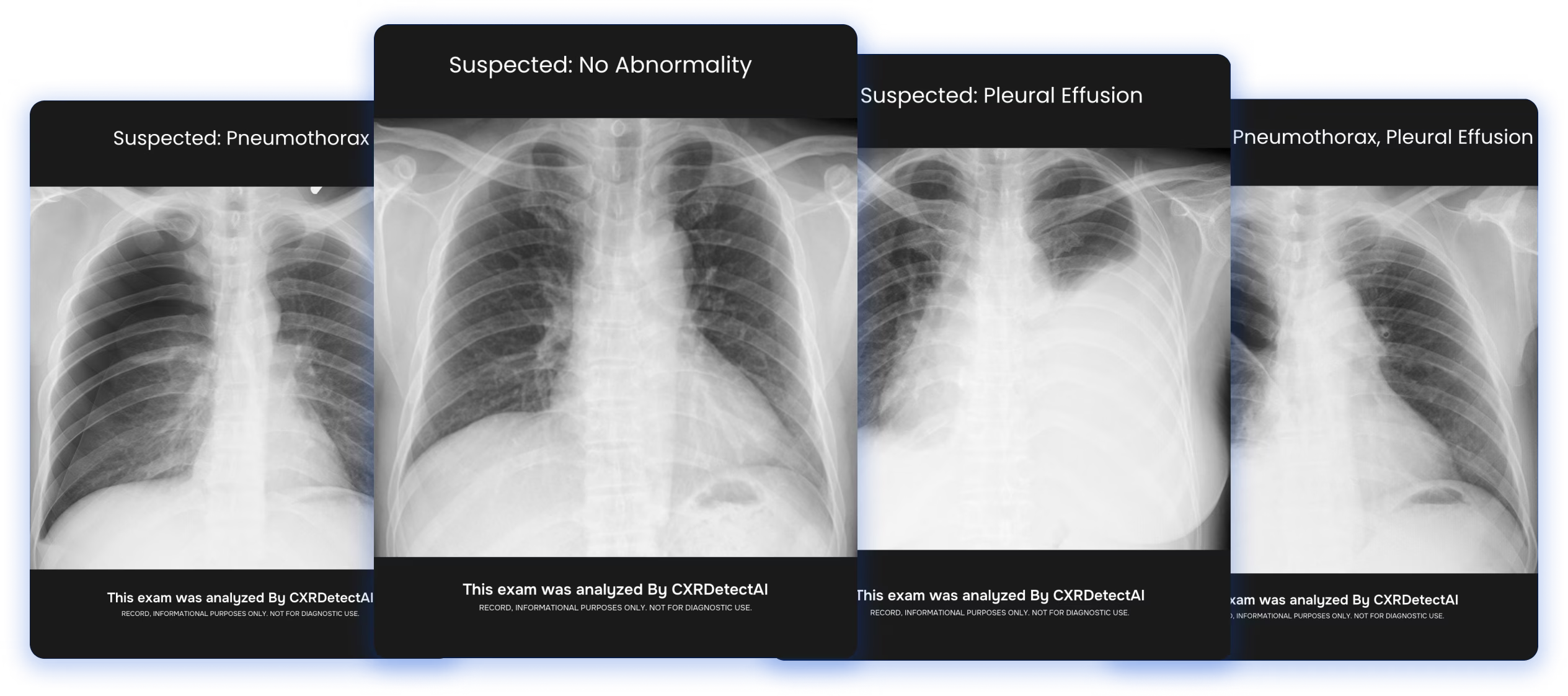
Enhancing precision and speed in critical chest X-Ray diagnosis.